Why I'm Losing Trust in the Institutions
The CDC came scarily close to adopting a plan that would, according to its own models, have killed thousands of Americans.
 |

Who should be first in line to get the vaccine against Covid-19?
These kinds of decisions are never easy, and there are many competing considerations. Highly trained moral philosophers can have deep disagreements about them. Though I myself have studied ethics and political philosophy for much of my academic career, I am deeply grateful that I don't have to make those judgment calls. But for all of those difficulties, there are also some bedrock principles on which virtually all moral philosophers have long agreed.
The first is that we should avoid “leveling down” everyone’s quality of life for the purpose of achieving equality. It is unjust when some people have plenty of food while others are starving. But alleviating that inequality by making sure that an even greater number of people starve is clearly wrong. The second is that we should not use ascriptive characteristics like race or ethnicity to allocate medical resources. To save one patient rather than another based on the color of their skin rightly strikes most philosophers—and most Americans—as barbaric. The Centers for Disease Control have just thrown both of these principles overboard in the name of social justice.
In one of the most shocking moral misjudgments by a public body I have ever seen, the CDC invoked considerations of “social justice” to recommend providing vaccinations to essential workers before older Americans even though this would, according to its own models, lead to a much greater death toll. After a massive public outcry, the agency has adopted revised recommendations. But though these are a clear improvement, they still violate the two bedrock principles of allocative justice—and are likely to cause unnecessary suffering on a significant scale.
Since states will now have to decide whether to follow the CDC’s recommendations, the fight for a just distribution of the vaccine is not yet over. At the same time, the past days have already taught us two lessons that sum up some of the most worrying developments of the past years: The attack on philosophically liberal principles has by now migrated from leafy college campuses to the most important and powerful organizations in the country. And, in part as a result, it is getting harder and harder to trust institutions from the CDC to the New York Times.
To learn more about Persuasion, read our founding manifesto.
On November 23rd, Kathleen Dooling, a public health official at the CDC, gave a presentation to the Advisory Committee on Immunization Practices (ACIP), which is tasked with developing the recommendation on who should first get access to the vaccine against Covid. In a stark departure from the course of action adopted in virtually every other developed democracy, Dooling recommended that 87 million essential workers—a very broad category including bankers and movie crews as well as teachers or supermarket cashiers—should get the vaccine before older Americans, even though the elderly are much more likely to die from the disease. The committee unanimously accepted the recommendations.
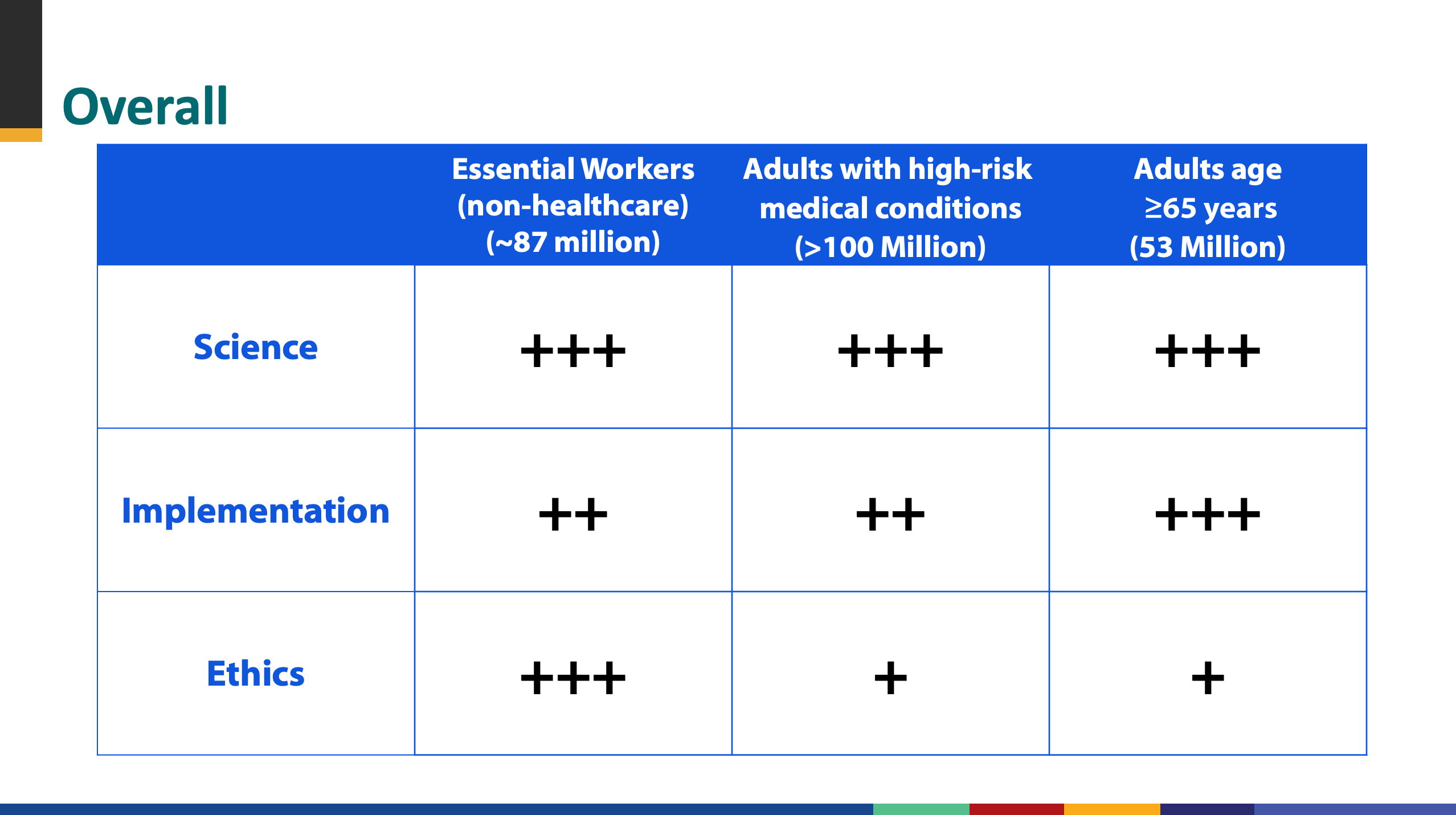
Dooling’s presentation laid out three different metrics for evaluating whether 87 million “essential workers” or Americans over the age of 65 should be next in line: feasibility, science, and ethics. According to the CDC's own evaluation, considerations of feasibility give us reasons to prioritize older Americans. This makes sense. It is both difficult to determine who should count as an essential worker and to communicate to people who do fall into that category that they are eligible. A straightforward age cut-off makes it easier to decide who's in and reach the target population. As a result, prioritizing the older 65s leads by this metric.
Considerations of “science” also seemed to point in the same direction. As the presentation acknowledged, the likelihood of dying from Covid strongly depends on age. According to the CDC’s model, prioritizing essential workers over the elderly would therefore increase the overall number of deaths by between 0.5% and 6.5%. In other words, it would likely result in the preventable deaths of thousands of Americans.
And yet, the presentation concluded that science does not provide a reason to prioritize the elderly. For, as Kathleen Dooling wrote in one of the most jaw-dropping sentences I have ever seen in a document written by a public official, differences in expected consequences that could amount to thousands of additional deaths are “minimal.”
This allowed Dooling to focus on “ethical” principles in selecting the best course of action. Highlighting the most important consideration in red, Dooling emphasized that “racial and ethnic minority groups are underrepresented among adults > 65.” In other words, America’s elderly are too white to be considered a top priority for the distribution of the vaccine against Covid. It is on this basis that ACIP awarded three times as many points to prioritizing the more racially diverse group of essential workers, making the crucial difference in the overall determination. Astonishingly, the higher overall death toll that would have resulted from this course of action does not feature as an ethical reason to prioritize older Americans.
In the days after ACIP published its preliminary recommendations, barely any epidemiologists or health officials publicly criticized its findings or its reasoning. But thankfully, prominent journalists like Zeynep Tufecki, Matt Yglesias and Nate Silver publicly made the case against them. (So did I.)
It is, all of us acknowledge, very important to ensure that members of ethnic minorities are not excluded from access to the vaccine on the basis of their race. But to prioritize a 23-year-old Latino Uber driver who is very likely to weather infection with Covid over an 80-year-old white retiree who is likely to die from it because the former is part of a group that includes marginally more brown people and the latter is part of a group that includes marginally more white people is to inscribe racial discrimination at the heart of American public policy in an astonishing manner.
It gets even more shocking. The difference in the percentage of white people across age groups is comparatively small. The difference in the percentage of infected people who succumb to Covid across all age groups is massive. Giving the vaccine to African-American essential workers before elderly African-Americans would likely raise the overall death toll of African-Americans even if a somewhat greater number of African-Americans were to receive the vaccine as a result.
In other words, the CDC was effectively about to recommend that a greater number of African-Americans die so that the share of African-Americans who receive the vaccine is slightly higher. In blatant violation of the “leveling down objection,” prioritizing essential workers in the name of equality would likely kill more people in all relevant demographic groups.
As criticism of the recommendations mounted, epidemiologists mostly circled the wagon. But thankfully, the pressure was too strong to ignore. At a meeting that had, before the mounting controversy, been expected to rubber-stamp the recommendations that had already been unanimously accepted, ACIP changed course. It now suggested a more complicated scheme. Once medical workers had received the vaccine, both Americans over the age of 74 and essential frontline workers would be vaccinated; in a second phase, Americans over the age of 64 and the broader group of all remaining essential workers would get access to the vaccine.
Since over half of all deaths from Covid have so far occurred among Americans over the age of 74, this is an undoubted improvement over the initial guidance. But, for two reasons, it too probably sacrifices American lives on the altar of social justice. First, vaccinating Americans over the age of 74 over the same period of time as frontline essential workers will significantly delay when some of those who are at greatest risk will receive the vaccine. And second, starting to vaccinate Americans between the ages of 65 and 74 after 30 million frontline essential workers will still put a large group with a comparatively low risk of death ahead of a large group with a significantly higher risk of death.
Just how many additional deaths will result from the ongoing refusal to prioritize those who are at the highest risk of dying? The CDC won’t tell us. In the updated presentation, Dooling once again claims that the difference between the CDC’s preferred course of action and a more strictly age-based approach is “minimal.” But this time around, ACIP has hidden the ball. The updated guidance, which was adopted with a 11-1 majority on December 20th, no longer includes an estimate of how many more people are likely to die if states follow its recommendation.
Get our articles directly into your inbox, and support the work of Persuasion, by becoming a subscriber.
Over the past years, stories of campus craziness have frequently made the national news. Whenever some student group or another tried to stop a public figure from speaking at their university, or boycotted the local dining hall over the inauthentic nature of its sushi, many people understandably responded in a dismissive manner: “Activists on campus have always been a little silly,” they’d say. “This won't affect the real world.”
It is now clear that this was a serious misjudgment. Many of the trends that started on campus have rapidly taking over established institutions, from Google to the Centers for Disease Control. Perhaps the most dangerous of these is that many professionals now fear to oppose any proposal that is presented, however implausibly, in the language of social justice—even if its foreseeable consequence is to kill a greater number of African-Americans in the name of “ethics.”
America’s botched guidance on who gets the vaccine first should, once and for all, put the idea that the excesses of wokeness are a small problem that doesn't affect important decisions to bed. But if it has shaken me to the core, it is in part because this sad saga also showcases yet another depressing conclusion.
By disposition, I trust the functioning of establishment institutions and the decent intentions of my compatriots. In a country with rapidly falling social trust and growing political dysfunction, I try to hold on to my belief that some key organizations are doing their best. Until a few years ago, it was obvious to me that I can trust what is written in the newspaper or what I am told by public health authorities.
Now, I am losing that trust. I still believe that most people, including the journalists who write for established newspapers and the civil servants who staff federal agencies, are the heroes in their own stories. They genuinely mean well. And yet, I no longer trust any institution in American life to such an extent that I am willing to rely on its account of the world without looking into important matters on my own.
The reasons for this mistrust are perfectly encapsulated in the reports that mainstream newspapers published about the CDC’s recommendation. The write-up in the New York Times, for example, barely mentions the committee’s last-minute change of heart. A faithful reader of the newspaper of record would not even know that an important public body was, until it received massive criticism from the public, about to sacrifice thousands of American lives on the altar of a dangerous and deeply illiberal ideology.
Yascha Mounk is the Founder of Persuasion.
____________________________________________________________________
How the Centers for Disease Control Went Woke
A look at the experts and the arguments that persuaded a government agency to prioritize 'equity' over saving lives
In 2015, Dayna Bowen Matthew, the dean of George Washington University Law School, published a paper concerning racial disparities in health care. She traced those disparities back to the Founding Fathers and argued their persistence today reflects the "structural violence" of American society.
Matthew was 1 of 11 people who helped draft the Centers for Disease Control's ethical framework for allocating COVID-19 vaccines. She is also listed as a "health equity" consultant to the Advisory Committee on Immunization Practices, which voted in November to vaccinate essential workers before the elderly, partly on the grounds that the elderly skew white—only to pull back Sunday in the face of outrage from across the political spectrum.
The committee openly acknowledged that its initial plan would result in more deaths than "vaccinating older adults first." But, the panel said, the plan would reduce racial disparities—something they deemed more important than saving lives—because essential workers, unlike adults over 65, are disproportionately black and Hispanic, the two groups that have borne the brunt of the pandemic.
How did the committee reach that conclusion? According to meeting minutes, presentation slides, public statements, and even civil-rights directives, the now-scuttled plan didn't come out of thin air. Rather, it reflects the reductive, racialist worldview that is rapidly gaining ground in education, media, nonprofits, and now the U.S federal government—a worldview with concrete policy implications and concrete human costs.
That policy agenda was seeded by outside consultants like Matthew, who told the New York Times that racial inequality "requires us to prioritize by race." But it was also seeded by the CDC itself, which in September hosted a series of trainings on "racism, sexism, and other systems of structured inequality," in direct violation of President Trump's executive order barring such programs from government agencies. And it was even seeded by the chairman of the CDC committee, José Romero, who said in July that minorities "need to be moved to the forefront" of the vaccination line.
The result was an explicitly race-conscious plan that would have prioritized shrinking the case gap between races over saving the most lives.
This plan contained glaring double standards, such as an assumption that age-based policies would be discriminatory but that race-based ones wouldn't be. It relied on omission, distortion, and equivocation to make a highly contentious judgment seem self-evident, building bureaucratic consensus upon shaky foundations that were anything but apolitical or science-based.
That consensus coalesced in September, when committee members met to discuss their framework for "vaccine equity and prioritization."
At the meeting, Sara Oliver, an epidemiologist with the CDC, delivered a presentation on the criteria the government should consider when developing a plan for rolling out a coronavirus vaccine. She began by reviewing three other frameworks—from the World Health Organization, the Johns Hopkins Bloomberg School of Public Health, and the National Academies of Science, Engineering and Medicine (NASEM)—on which her working group had drawn in formulating its own principles.
"Equity," Oliver emphasized, was a "crosscutting consideration for all three frameworks," suggesting that the CDC would be in good company if it prioritized that value.
But all three frameworks also considered harm reduction to be an important goal. In fact, they tended to prioritize saving lives over reducing disparities, a point Oliver either ignored or overlooked.
For example, although the Hopkins framework includes several throat-clearing paragraphs about the impact of "structural racism," it concludes by suggesting adults 65 and older receive vaccinations before most essential workers—the "primary reason" being that "their prioritization would likely avert the greatest overall harm."
But the CDC's framework adopted different priorities. Of its five proposed principles—maximize benefits and minimize harms, equity, justice, fairness, and transparency—two explicitly mention racial health disparities.
"The equity principle," Oliver said, according to meeting notes, will "make sure that vaccine allocation reduces, rather than increases, health disparities," while the "fairness principle includes a commitment to … not exacerbating existing disparities in health outcomes."
The result was a kind of moral double counting, in which closing disparities promoted two separate values, whereas saving lives promoted just one. As phrased, equity and fairness sound like they are at odds with harm reduction: If vaccinating by age minimized deaths across all racial groups, but widened the gap between racial death rates, the principles seem to rule out that strategy, since it would increase racial disparities overall.
The Washington Free Beacon asked 13 members of the CDC advisory committee whether this was an accurate reading of its framework. Not a single one answered the question, though Kathy Kinlaw, the group's sole "ethics consultant," said she thought "mitigating health inequities" would "minimize harm—and maximize benefits—for all."
The CDC also expressed concern that vaccinating by age would amount to immoral—and potentially illegal—discrimination. The evidence its experts cited, however, arguably favored doing just that.
One graphic from Oliver's presentation, used to illustrate the trade-offs of prioritizing the elderly, cites a statement from the American Geriatric Society that "age should never be used to exclude someone from a standard of care, nor should age ‘cut-offs' be used" to allocate scarce supplies. It also notes that the Health and Human Services Office for Civil Rights had objected to triaging ventilators by age at the start of the pandemic.
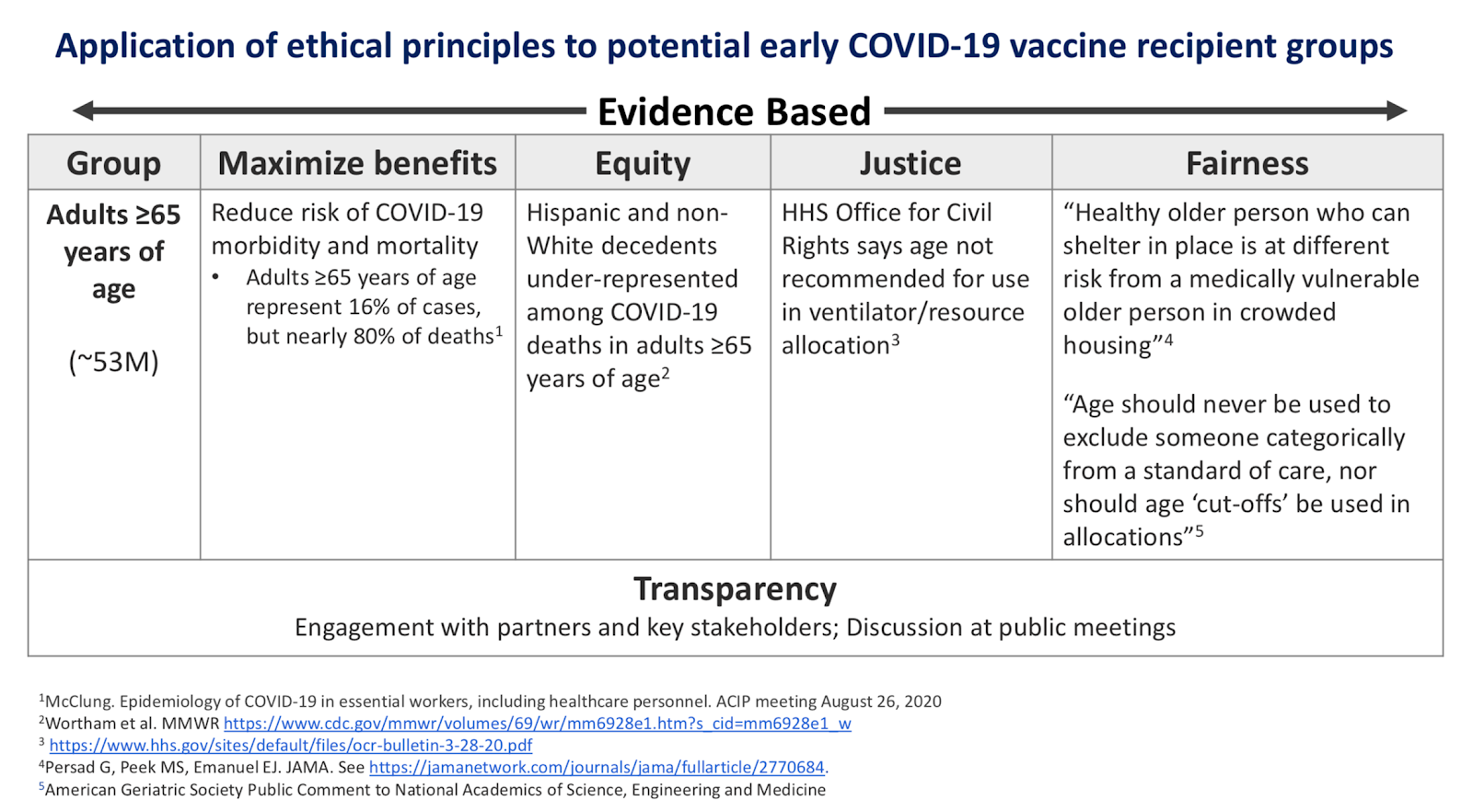
Slide 32 of Oliver's presentation, "Overview of Vaccine Equity and Prioritization Frameworks," September 22, 2020
The HHS office, however, was worried about triage plans that discriminated against the elderly, "such that older persons might automatically be deemed ineligible for life-saving care without any individualized assessment." The president of the American Geriatric Society concurred, saying that age-based criteria "disfavo[r] older adults regardless of their function and health relative to COVID-19."
The CDC committee thus took two statements that championed the interests of the elderly and used them to justify a plan that would disproportionately kill senior citizens—implying that age-conscious alternatives were discriminatory, even as the race-conscious plan passed with unanimous support at a subsequent meeting.
All of this—the exclusions, the contradictions, the moral redundancies—helped disguise the agenda that it justified, giving unscientific value judgments an air of scientific assuredness.
The backlash against those judgments hasn't contained the ideology that gave rise to them. Marcella Nunez-Smith, a co-chair of Joe Biden's COVID-19 advisory board, commended the experts at the CDC for "taking political interference out of the process" and for "their grounding in inequity." Like them, she seems not to have realized the irony.
No comments:
Post a Comment